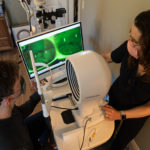
Dr. Periman working with a patient to capture images. She says this software’s impressive anterior imaging capacity continues to help her deliver a hybrid model of care that incorporates both in-office and virtual appointments.
Sponsored Content
By Laura M. Periman, MD
June 8, 2022
The pandemic significantly tested every industry. Healthcare, including eyecare, was no exception.
I decided to launch my dry eye specialty practice in April 2020 in the depths of the pandemic’s first wave. A silver lining was the forced workarounds many of us needed to come up with, and how those workarounds then revolutionized the way we do things.
For eyecare providers, that meant finding an alternative to seeing patients in the office, especially since our patients still needed our help.
I’ve always been generally tech-savvy, and I enjoy exploring new technologies. When we were cobbling together our new eye institute, for instance, we had to stack multiple IT solutions as we were unable to find fully integrated scheduling, practice management, EHR and communications platforms. I didn’t want to go with the big-name electronic health systems because as a new, small clinic, we wouldn’t be able to get the support we needed in the event of tech problems, and they were way overpriced. That meant we had to look at cost-effective alternatives.
Given patients’ needs and requests, we sought to offer telemedicine from the outset in the interest of COVID safety. We had clinic space by June 5, 2020, but we have found telemedicine to be so effective, efficient and satisfying for patients and staff that we have kept it.
The workflow of a patient booking a telemedicine appointment with us involves the patient completing all the on-boarding forms available on our website. These HIPAA forms include dry eye questionnaires, risk factor identification and detailed medical history. An unforeseen benefit of these extensive forms has been the impact on patient education. In the process, patients develop the vocabulary they need to tell me what they are experiencing. It’s a fantastic way of beginning our patients’ journey, and I’ve been so impressed with how people have been able to effectively and efficiently communicate their dry eye story in their own words.
The active listening during extensive history intake facilitates accurate diagnosis and initiation of therapy (OTC and prescription). We help the patient “connect the dots” with patient education and discussions of potential treatment options.

Imaging Dr. Periman achieved through use of Advanced Ophthalmic Systems (AOS) technology. She says having the ability for this kind of imaging has changed how she practices.
Informed consent links are included in the after-telemedicine visit summary. Advanced in-office testing confirms the diagnosis and candidacy for in-office treatments. A fully integrated treatment plan is in place by the end of the first in-person visit. This goes a long way toward putting patients at ease and slowing the process down, which makes for a more relaxing experience than that of a typical doctor’s office encounter.
In addition to creating an engaging patient experience, our staff reaps the rewards of telemedicine by streamlining intake forms and chart-building, which frees up significant time. This is huge for our small boutique practice with a lean workforce. The added efficiency means we’re able to achieve economies of scale and see more patients.
Digital Imaging Using AOS Objective Analysis
A telemedicine platform is built into Advanced Ophthalmic Systems (AOS), a software I began using before the pandemic to leverage its advanced anterior imaging capabilities. This new digital imaging technology revolutionized our ability to explain to patients exactly what’s going on with their condition and objectively measure important metrics like quantifying fluorescein staining as well as conjunctival edema and injection.
In eyecare, imaging tells a story worth a thousand words. Digital imaging using AOS’ objective grading technology enables us to demonstrate improvements and provide hope to patients. Sometimes just being able to visualize changes and improvements can encourage the patient that they are on the right path, making them more likely to continue with the recommended treatment pathway.
In clinical practice, precision image analysis offers a significant advantage over traditional grading scales which are fraught with inter- and intra-observer variability. With our clinical research, the power of quantifying corneal staining and conjunctival injection facilitates finding statistical significance with a smaller number of patients, which saves studies time and money. I would love to see more objective analysis of images in clinical research. I think it would be helpful in bringing new innovations to market since there is still so much unmet need in the dry eye space.
A Hybrid Approach to Digital Eyecare
Effectively encouraging patients to stay on course with recommended therapy lends itself to a blend of remote and in-office care. This hybrid approach allows us to serve a wider range of patients. Regardless of whether a patient can travel to our clinic, I can monitor their progress, even if they’re not in our area, and keep track of how they’re responding to the treatment pathway. There are certain prescriptions I’m comfortable with issuing via telemedicine, but even when I’m not, telemedicine is a great way of starting the integrated treatment plan.
For example, one of my remote patients, an educated person with severe dry eye who works in medicine, had been skeptical of the possibility that advanced treatments could help. Their perspective changed after I shared AOS analyzed images of their eyes (see image above). Everything then made total sense, and they were put at ease.
Our industry has a long way to go in utilizing these new digital eyecare technologies, but the positive impact on patients and practices is already apparent. The response from even the least tech-savvy patients is positive. Our referring colleagues have enhanced confidence that we can accurately diagnose, expertly treat and track the progress of their patients.
The ability to offer these new technologies has been a differentiator for our practice.
 Laura M. Periman, MD, is the Founder and Director of Dry Eye Services and Clinical Research at Periman Eye Institute in Seattle, Wash. She is an expert in dry eye disease treatment, and specializes in the medical treatment of corneal surface problems and minor external and ocular surface procedures.
Laura M. Periman, MD, is the Founder and Director of Dry Eye Services and Clinical Research at Periman Eye Institute in Seattle, Wash. She is an expert in dry eye disease treatment, and specializes in the medical treatment of corneal surface problems and minor external and ocular surface procedures.
























