Office surgery in progress in the office of ROB Professional Editor Laurie Sorrenson, OD, FAAO. Dr. Davis says it’s essential to get the basics down of coding for office surgeries.
Coding for office surgery to ensure accuracy and timely reimbursement.
Nov. 29, 2023
By Mark K. Davis, OD
As optometry increases its scope of practice across the nation, office surgery is becoming more common. Medical optometry is beginning to comprise more of the gross revenue of optometric practices, especially as online competition for contact lens and glasses sales increases. Also, as many of today’s new graduates choose to do residencies in ocular disease, they may not be satisfied with practicing traditional optometry. With all of that in mind, let’s take a look at how to properly code for office surgery.
Global Surgical Package
Here is what is included in the Global Surgical Package according to the CPT Manual:
- One E/M service the day before or day of surgery
- Local or topical anesthetic
- Immediate post-operative care
- Dictate operative notes
- Talk with family or physicians
- Writing orders
- Evaluating patient in recovery area
- Post-operative follow-up that occurs directly after the procedure
- Major surgery – 90 days
- Minor surgery – 0 to 10 days
Many optometrists still do not know that you cannot charge for an office visit the same day you perform a surgical procedure. It is included in the reimbursement for the surgical code. There are exceptions, but they are rare. One that I can think of is if a patient is coming for an IOP check and happens to mention that one of their eyes has been feeling scratchy. When checking the IOP by Goldman tonometry, you also note trichiasis in the affected eye. The coding would be as follows:
92012 or 99213 – 25 H40.11XX (depending on stage of POAG)
67820 epilation, forceps only H02.05X (depending on which eye and eyelid)
The 25 modifier, as you may recall from a previous article, is appended on the office visit code and indicates a significant, separately identifiable E/M service on the same day of a procedure.
Patient’s Chart
According to Medicare; Code of Federal Regulation (CFR) Section 482.51(b)(6), here is what the patient’s chart must contain:
- Name & ID #
- Date and time of surgery
- Properly executed informed consent
- Name of surgeon(s) and assistant surgeon(s)
- Pre-operative/post operative reports
- Name/code of specific surgical procedure
- Type of anesthesia administered
- A description of surgical procedure/techniques, findings and tissue removed or altered, device implanted
- Outcome statement – complications, if any
- Discharge instructions given to patient
- Signature of the surgeon
From a legal standpoint, the most important single point listed above is the signed Informed Consent. I have been an expert witness on a few malpractice cases. Not having a signed Informed Consent can really set the defense counsel back. Simply having a signed Informed Consent will, in many cases, dissuade an attorney from even taking the case.
Other Articles to Explore
Common Surgical Codes Used in Optometry
Here is a list of the most common ocular surgical codes and the global fee period of each. It is not all-inclusive. A global fee period is the number of days that no additional office visit may be charged by the provider for the initial surgical code. An office visit may be charged for an unrelated problem that arises.
For example, if you removed a lid lesion by chemical cautery (67850, global fee period is 10 days) and the patient developed an allergic conjunctivitis from ragweed and needed to be treated with a steroid within the 10-day global fee period, you could charge an office visit with the appropriate diagnosis code and using the 25 modifier.
- 65205 – foreign body removal, conjunctiva, superficial (0 days)
- 65210 – foreign body removal, conjunctiva, embedded (0 days)
- 65222 – foreign body removal, cornea, with slit lamp (0 days)
- 65286 – repair of laceration, cornea or sclera, glue (0 days)
- 65435 – removal of corneal epithelium (0 days)
- 65778 – placement amniotic membrane on cornea, without sutures (0 days)
- 67820 – excision of chalazion, single (10 days)
- 67820 – epilation, forceps only (per eye) (0 days)
- 67840 – excision of lesion of eyelid (except chalazion) without closure (10 days)
- 67850 – chemical cautery, lid lesion up to 1 cm (10 days)
- 67938 – removal of embedded foreign body, eyelid (10 days)
- 68530 – removal foreign body, lacrimal passage (10 days)
- 68761 – closure of lacrimal punctum, plug, each (10 days)
- 68020 – incision of conjunctival, drainage of cyst (10 days)
- 68801 – dilation of lacrimal punctum, with or without irrigation (10 days)
- 68810 – probing of nasolacrimal duct, with or without irrigation (10 days)
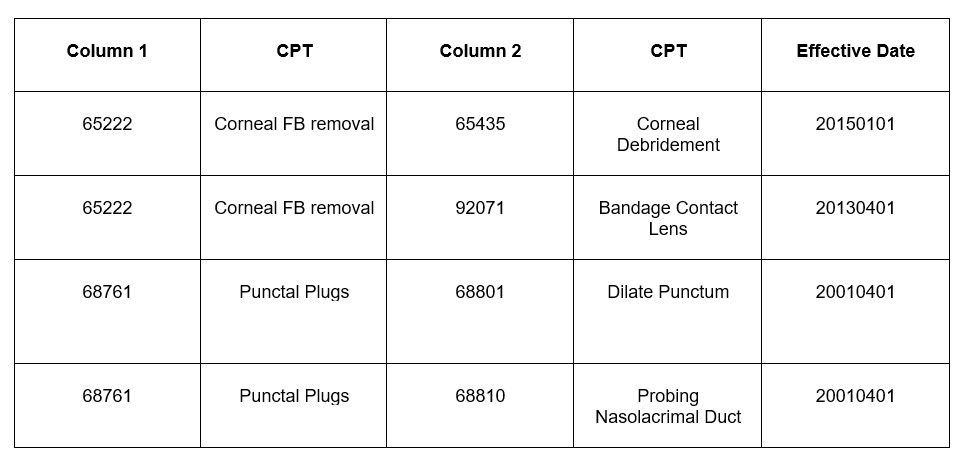
National Correct Coding Initiative (NCCI)
Just as some special diagnostic tests cannot be performed on the same day due to the NCCI edits, the same holds true for certain surgical codes. The following chart gives some examples of surgical codes that will not be paid together on the same day of service. This is according to the National Correct Coding Initiative Coding Policy Manual for Medicare Services (Coding Policy Manual). I also included CPT 92071 fitting of contact lens for treatment of ocular surface disease, commonly called a bandage contact lens. Some doctors still do not know you CANNOT charge for applying a bandage contact lens when removing a corneal foreign body.
Hopefully this article has been helpful, and possibly clarifies correct coding for office ocular surgery. This is an area I believe will become more important as our great profession evolves over time. Happy coding!
 Mark K. Davis, OD, is a Therapeutic Optometrist and Optometric Glaucoma Specialist, Diplomate, American Board of Optometry, Adjunct Assistant Professor, University of Houston College of Optometry and Chief of Optometry, 147th Medical Group. He is Lt Col, Texas Air National Guard, Ellington Field JRB, Houston, Texas. To contact him: mkdavisod@gmail.com
Mark K. Davis, OD, is a Therapeutic Optometrist and Optometric Glaucoma Specialist, Diplomate, American Board of Optometry, Adjunct Assistant Professor, University of Houston College of Optometry and Chief of Optometry, 147th Medical Group. He is Lt Col, Texas Air National Guard, Ellington Field JRB, Houston, Texas. To contact him: mkdavisod@gmail.com
























