By Mark Wright, OD, FCOVD,
and Carole Burns, OD, FCOVD
 Jan. 9, 2019
Jan. 9, 2019
Taking a thorough history of each patient’s health is essential to delivering quality care. Here’s how to ensure you are accurately coding for that history.
There are three histories that should be taken on every patient. These are the demographic history, the lifestyle history and the medical history. For coding and billing purposes, the medical history is most important.
Today will explore the medical history for the 99000 E/M codes.
There are four parts to the medical history: Chief Complaint, History of Present Illness (HPI), Review of Systems (ROS), and Past, Family, and Social History (PFSH). Each of these components need to be explored with the patient and documented appropriately for coding and billing purposes. (From a clinical standpoint, document elements that help you best manage patient care.)
Chief Complaint
According to the CPT coding rule book “a chief complaint is a concise statement describing the symptom, problem, condition, diagnosis, or other factor that is the reason for the encounter, usually stated in the patient’s words.” The chief complaint is the reason for the visit. This is important because the reason for the visit (i.e.: the chief complaint) either opens or closes the first gate for medical reimbursement. If the reason for the visit is not a medical sign or symptom, or ongoing care for a medical condition, then the first gate for medical reimbursement is closed.
Acceptable reasons for the visit which open the first gate for medical reimbursement would be: burning eyes, crossed eyes, distorted vision, double vision, dry eyes, eye pain, flashes, floaters, halos, red eye and watery eyes. Note that the examples given here for chief complaint are two words or less. If you’re using more than two words to describe the chief complaint, odds are that you are including HPI history. An example would be “red right eye.” Instead, the chief complaint would be better identified as “red eye” because “right” in this example is really the answer to the HPI element Location.
Before you can identify the actual level of medical history you have taken, you must first determine the level of HPI, ROS and PFSH you have taken. Here’s how you do that.
Other Articles to Explore
History of Present Illness
The History of Present Illness is a chronological description of the development of the patient’s present illness from the first sign/symptom or from the previous encounter to the present. The History of Present Illness has eight elements: Location, Quality, Severity, Duration, Timing, Context, Modifying Factors and Associated Signs & Symptoms.
It’s interesting to note that auditors do not evaluate your answers, they simply count how many elements you have answered. That gives you significant flexibility in your answers. For example, for the severity element you could answer using a mild, moderate or severe scale. You could also answer the severity element using a 1 to 10 scale, where 1 is low severity and 10 is the highest severity. You could also use a low, moderate or high, answer for this element. The auditor is not worried about what you answered, but only how many elements you documented.
The History of Present Illness has only two levels: Extended and Brief. To code an Extended HPI, you need to document answers to at least four of these eight elements. If you answer more than four of the eight elements, it is still an Extended HPI. You must code at least one of the elements in order to have a Brief HPI level.
Review of Systems
Review of Systems has 14 elements and three possible levels. The elements are:
1) Constitutional Symptoms (Fever, Weight Loss)
2) Eyes
3) Ears, Nose, Mouth, Throat
4) Cardiovascular
5) Respiratory
6) Gastrointestinal
7) Genitourinary
8) Musculoskeletal
9) Integumentary (Skin and/or Breast)
10) Neurological
11) Psychiatric
12) Endocrine
13) Hematologic/Lymphatic
14) Allergic/Immunologic
The ROS levels are determined by how many of the 14 systems you document answers to. A Problem Pertinent ROS is achieved by documenting an answer to the one system directly related to the problem the patient is having. An Extended ROS is when you document answers to 2-9 of the 14 systems. A Complete ROS is when you document answers to 10 or more of the systems.
Ask symptoms of systems questions. For example, rather than ask, “Are you having respiratory problem?,” it is better to ask, “Do you experience shortness of breath?”
Past, Family, and Social History
Think of this as three separate histories: a Past History, a Family History, and a Social History. In the Past History you want to know about past illnesses, operations, prescribed medicine, injuries and treatment. In the Family History you are doing a review of medical events in the patient’s family, including diseases which may be hereditary or place the patient at risk. In the Social History explore employment, education, use of drugs, alcohol and/or tobacco.
There are two levels of PFSH: Complete and Pertinent. To have a Complete PFSH you need to document at least one answer for Past History, one answer for Family History, and one answer for Social History for a new patient. For an established patient, the criteria for a Complete PFSH is less. In the heat of battle in the clinic, rather than try to remember the difference between a new patient and an established patient for PFSH, just always document at least one answer for Past History, one answer for Family History, and one answer for Social History.
If you have documented just one answer for only one of Past History, Family History, or Social History, then you have a Pertinent level PFSH.
What level of medical history did you take?
Do you have a medical sign, medical symptom, or ongoing care, for a medical condition as your Chief Complaint? If the answer is no, then the gate to medical reimbursement is closed and it really doesn’t matter what level of medical history you took. But if the answer is yes, then we can proceed.
Use the following chart to determine the level of medical history taken.
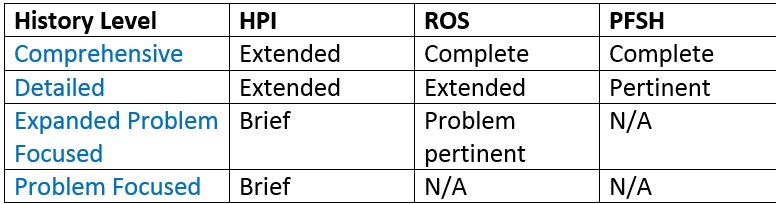
The easiest way to read this chart is to go to the lowest level of history that you documented, and that is the level of history that you have coded. Let’s do a few examples to make this clear.
If you have taken an Extended HPI, a Complete ROS, and a Complete PFSH, then this would be coded as a Comprehensive Medical History.
If you’ve taken an Extended HPI, an Extended ROS, and a Complete PFSH, then this would be coded as a Detailed Medical History.
If you’ve taken a Brief HPI, a Complete ROS, and a Complete PFSH, then this would be coded as an Expanded Problem Focused Medical History.
What if you have taken an Extended HPI, but you did not document anything for ROS or PFSH? Then, this would be coded as a Problem Focused Medical History.
To read more about coding the 99000 E/M exam, read this document and the reader should refer to CPT for the complete descriptors for E/M services and instructions for selecting the appropriate level of service.
References
i. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf


























