By Mark Wright, OD, FCOVD,
and Carole Burns, OD, FCOVD

May 3, 2017
A patient presents in your office with a corneal foreign body in the left eye. It’s the first time you’ve seen the patient with this problem (i.e. initial encounter). What diagnosis and procedure codes do you use? Let’s start with the diagnosis code.
What diagnosis code do you use?
Here are the options…
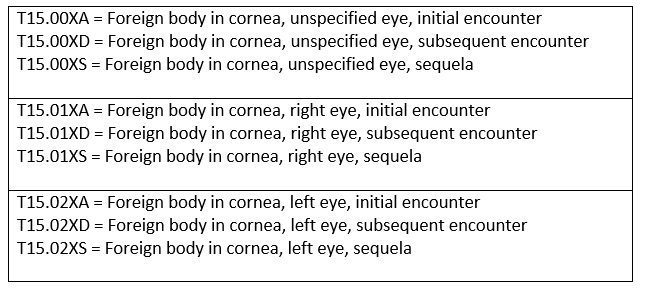
The “unspecified eye” codes should never be used. You are an eye specialist. You are supposed to know which eye contains the corneal foreign body. With that in mind, the choice becomes either right eye or left eye. The case we are considering is the left eye.
Looking at the chart above, the appropriate diagnosis code for the case we are considering is T15.02XA. The 2 in this code tells us it is the left eye (it would be a 1 for the right eye). The A in the code tells us it is an initial encounter (the other options are: D = subsequent encounter and S = sequela). The ICD-10 diagnosis code T15.02XA is foreign body in the cornea, left eye, initial encounter.
What procedure code do you use?
CPT code 65222 is removal of foreign body, external eye; corneal, with slit lamp.
65222 is a bundled code. That means if you have two or more foreign bodies in the same tissue in the same eye, on the same day, you can only bill once for the multiple foreign bodies. But, if you have both a corneal foreign body and a conjunctival foreign body in the same eye at the same time, then you can bill for both. In the case of both a corneal and conjunctival foreign body in the same eye at the same time, you would use the CPT codes of 65222 and 65205 using the appropriate diagnosis code with each procedure code.
It is important to note that CPT code 65222 is a per eye code, so the other case to consider is if you have a corneal foreign body in the right eye and the left eye at the same time. In this case, you can bill for the corneal foreign body removal in each eye using the -RT and the -LT modifiers with the procedure code. The multiple surgery rule would apply, so you would also use the -52 modifier on the second eye.
The CPT code to use for the case we are considering is 65222-LT.
Documentation suggestions
Make sure your documentation identifies how many corneal foreign bodies exist, the exact location with a note of the specific tissue involved (e.g.: corneal or conjunctival), as well as the depth of each foreign body.
Instead of using a SOAP notes (i.e.: Subjective, Objective, Assessment, Plan) approach for documentation, it is best to use a Surgical Notes approach. The Surgical Notes approach contains the following elements:
1) Describe the Medical Condition
2) Describe Previous Treatment Attempted
3) Document Informed Consent
4) Describe the Procedure
5) Outcome Statement
6) Discharge Instructions
Can I bill an exam code in addition to the 65222 code?
The answer is yes and no.
The answer is no if during your examination of the patient you discover the corneal foreign body, it is the only problem you discover, and you remove it the same day. “The initial evaluation for minor surgical procedures … is always included in the global surgery package” (Medicare Claims Processing Manual, Chapter 12, Section 40.1.B).
The answer is yes if you discover another problem that is unrelated to the minor surgical procedure that needs to be addressed during the same office visit. For example, if you identify a blepharitis and a corneal foreign body, then you would code for the corneal foreign body removal with the diagnosis of corneal foreign body and also code a 99000 E/M code with the -25 modifier with the diagnosis of blepharitis.
The -25 modifier is a significant, separately identifiable evaluation and management service by the same physician on the same day of the procedure or other service.
In the case where you are billing an exam code with the surgical code, the E/M documentation must “stand alone” from the surgical procedure and be unrelated to the surgical procedure. To be clear to anyone auditing your records, separate your E/M documentation from the surgical procedure documentation. Make sure your electronic medical record is able to do this.




















